Top 5 Things We Learned in the Use of Video in Health and Social Care
During the lockdown, we have seen wider engagement with video calling in healthcare. But, in this article Consult Red’s Adam Hoare argues that this adoption of video is not guaranteed in the future just because it has demonstrated it’s worth during COVID.
Our experience indicates that service and support are key aspects of embedding remote care into practice.
By integrating video into our existing healthcare provision there’s a lot to be gained both for the healthcare industry and for patients. These new ways of working need to be captured and the evidence collected in support of a more enlightened commissioning approach that values a wider range of outcomes.
Between 2006 and 2016 Consult Red was instrumental in developing and deploying a video communication system to support clinician to clinician and clinician to patient virtual visiting. It also connected social care and community services to health care and facilitated family communication and support.
The recent rise in the use of off-the-shelf video products provides a timely opportunity to revisit what was learned and consider features that support wider adoption of remote care and its evaluation. The goal of the approach we adopted was to support health and social care integration through improved communication. The technology platform was evolved in collaboration with a wide range of partners.
The first learning point relates to the development of functionality in response to actual practice in the field.
1. Develop the solution in collaboration with Practice
When video replaces a consultation that would have taken place in person it is just providing an alternative communication method such as the telephone. This has benefits in the current pandemic environment but can be made much more compelling by considering the use of video as a way of changing practice. Figure 1 shows some of the considerations we undertook when developing the video capability to support new ways of working.
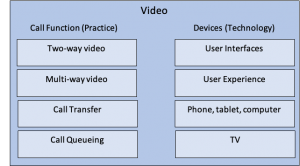
One of the key things addressed by our approach was the user interface and user experience for the patient in engaging with the video. We developed a set-top box that turned the TV into the communication device. Using a camera and a simple remote control, the video experience in the home became more natural. This enabled patients to be supported through virtual ward rounds where people were at home and took place in a ward round from their living room.
In collaboration with consultants and nurses, we went on to develop a range of functionality that enabled new ways of working. The implementation of virtual ward rounds inspired us to develop virtual waiting rooms where people could wait for their consultation. We also developed call transfers to facilitate call handling and onward routing to the appropriate response. This flexibility in call management resulted in several hospitals allowing long-term conditions patients to call in during office hours. They provided ad hoc support to offer responsive care to people in their own homes.
Later on, we implemented multi-way video calling such that multi-disciplinary team meetings could be held with people in their own home and even with family members conferenced in from their home. These multi-way calls facilitated the participation of multiple professionals in support of a person and their family.
A further extension of this multi-way capability was to provide virtual referrals. A GP, for instance, could offer a person a same-day consultation with someone in secondary care from their surgery by coordinating with the local hospital. With the ability to shorten waiting times and support ad hoc consultations much of the administrative overhead and slow appointment communications were avoided.
The solution was developed to be available on a range of different technologies including the TV, tablets, laptops, smartphones and desktop computers such that the right interface could be provided for each user of the system.
2. Service and Support
Free and commodity video calling has been available for some years but has not resulted in widespread adoption or embedding in clinical practice. During the lockdown, driven by the pandemic, we have seen wider engagement with video calling. The continued use of video is not guaranteed just because it has demonstrated utility in these difficult times. Our experience indicates that service and support are key aspects of embedding remote care into practice. Within service and support, we include the ongoing development of the technology in collaboration with front line care as well as having someone to call when problems occur.
Any credible remote care offer needs a service not only for support but also for customisation and development. In our experience care providers, when engaged in collaboration, quickly start to see how small changes could make the use of the technology more effective and ask for changes. As organisations we worked with engaged with remote care and its potential was revealed, the ability of the service to evolve was actively embraced resulting in new capabilities and integration with other systems. In order for remote care to catalyse transformational change, it must be able to evolve, and it must be actively and appropriately supported.
Often technology solutions are treated as IT projects and the responsibility for implementation and management falls to the IT department. This treats solutions as off-the-shelf product that just require implementing and the occasional update. For innovative and collaborative solutions, it is more successful if the supplier provides its own support as a service. However, this then leads to challenges over operational versus capital expenditure. Too often technology is seen as a predominantly capital expenditure with little consideration given to the ongoing operational costs that are required for the key aspects of service and support.
We consider that over and above the basic functionality such as video, service and support are a fundamental requirement for embedding, scaling and system change.
3. Security and Interoperability
Encryption of video and data is a fundamental requirement of communication systems used in care. A further consideration is the location of any servers that support the service with a requirement that data does not cross international borders. Further, the need to be able to communicate between GP surgeries and hospitals as well as over domestic broadband into people’s homes all bring challenges. Over time we developed support material for each set of stakeholders that gave examples of implementations across other care locations and how the security and interoperability across those networks was achieved. The development of multi-way video and call transfers added to the complexity of the considerations and required a steady accumulation of support material.
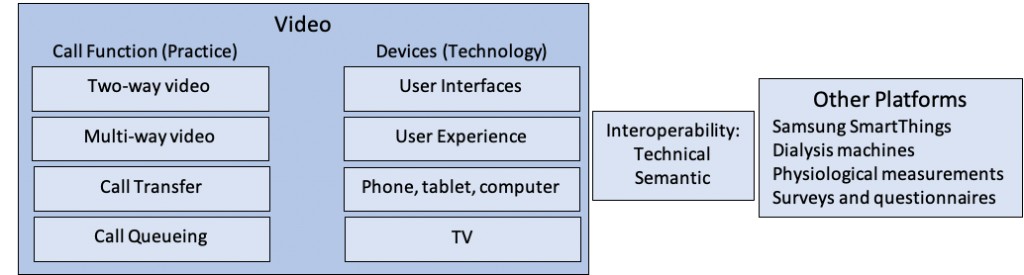
Communication technology provides a way to improve integration of care services. Interoperability with other platforms and devices offers a way to leverage other developments and better integrate data and reporting. We implemented a range of service developments that required interoperability with third-party systems. Figure 2 shows some of the platforms and devices we interoperated with.
Interoperability is often considered to be a predominantly technical issue. This is typically revealed to be a simplification once connectivity is established. Interoperability has two dimensions. The first is technical and relates to how two systems securely connect to each other. The second is semantic and relates what the shared data means.
Technical interoperability can be achieved through many means. Secure Application Programming Interfaces (APIs) are commonly used. Simple one-to-one connections can be accommodated by APIs as long as there is intelligence around failed connections and recovery to prevent data loss. In the complex world of health and social care, such simple connections are less useful. When dealing with many to many connections, secure messaging is more reliable and scalable.
Semantic interoperability relates to the meaning carried by data. There are a wide range of situations where semantic interoperability can be challenging.
Some of these include:
- Duplicate records
- Records that contain errors
- Missing data from records
- Variations in data coding (even across deployments of the same system).
- Interpretation of free text fields
Once technical interoperability is achieved there is usually a significant amount of work to cleanse and qualify the data to ensure that the systems are interoperating correctly. One of the recurring themes in care is the need to enter the same data on multiple systems sometimes with slight variations. This leads to a patchwork of data and the risk of the errors above being introduced.
During our work, we developed interoperability with several other platforms and devices. At the simplest level, this was represented by Bluetooth devices in the home such as pulse oximeters and weighing scales. We provided a way for clinicians to see the readout from the devices as part of a remote consultation. This concept was extended significantly with our collaboration with a renal department of a large hospital where we implemented a renal clinic at home.
This was in support of patients that undertook home haemodialysis. We installed the video capability along with an additional security device that allowed the connection of the dialysis machine to our secure service. In the hospital, we installed a second security device that allowed all of the readings from the dialysis machine to be securely communicated and stored in the hospital database. This meant that the patient could dialyse at home, undertake video consultations, receive support, as well as report physiological readings from home. This reduced travel and provided patients with a much better experience of care. It also provided the hospital with much richer patient data.
We developed interoperability with the Samsung SmartThings platform to improve waking night cover in a residential location for people with learning disabilities. The ability to detect movement at night along with the video support offered new ways of ensuring resident safety.
The interoperability with the platform that provided surveys and questionnaires was initially to integrate the Health Equalities Framework with our support for people with learning disabilities. It also supported our growing understanding about the role of context in the use of communication technology in care.
4. Context and Evidence
As we developed a range of interfaces and functionality to support new ways of working, we began to realise that the evidence for all of this new activity was not being collected. Because we were disrupting practice, the new ways of working enabled were not being recognised or characterised. After some years enabling new practice, we recognised that the communication platform needed to record the context of the activities it was facilitating. As shown in Figure 3 each new way of working sits within a context that must be captured in order to build the evidence base.
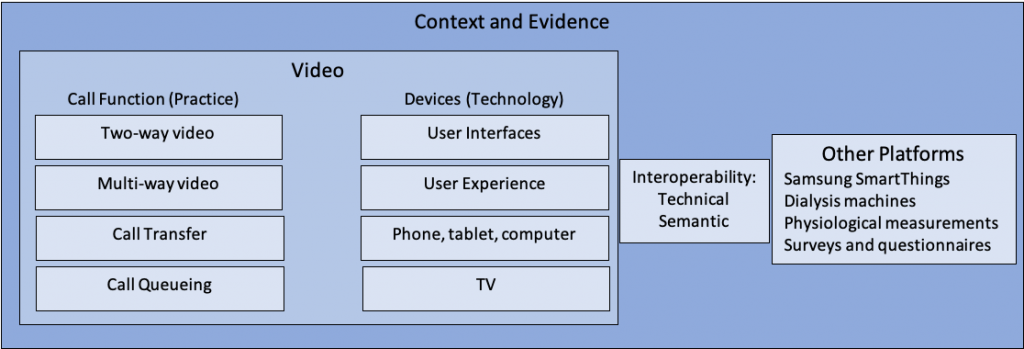
We began by capturing the context of consultations by allowing some free text to be entered during a call. Use of tick-boxes allowed feedback on the success of the call and technical issues to be recorded. We then introduced context-specific templates such that data specific to the type of call could be captured. The participants in the call and the call length were also key pieces of information that could be collected. Each remote consultation therefore collected timing, participation, pre-defined and free text data.
As the flexibility of video communication increased the need to track and monitor the system use grew. Building the data collection into the communication platform supports learning and evaluation.
5. Outcomes and the Economic Case
After a significant journey that first focussed on the technology in practice and then began to capture the context and activity we came to some key realisations:
- The people in front line care were actively interested in improving communication and adopting new ways of working – particularly when they were involved in developing the new approaches.
- The improved communication resulted in significant reductions in acute and routine activity in the care system.
- Engagement with families was improved using the communication technology. Often this resulted in better coordination with family members. The challenge was – under what circumstances the technology was made available to family members.
- The outcomes for the patient in having reduced travel and more immediate support were welcomed but were not recognised in the economics of commissioning.
- Communication technology did support more integrated care. The challenge routinely came down to who would pay for the service.
Conclusion
In the current situation, the use of video is driven by the risks involved in face-to-face interactions. Once these risks are diminished it is quite likely that people will snap back to familiar ways of working. The evidence from the pandemic experience so far is that video could play a positive part in care provision. Our experience is that there is much to be gained if the use of video is integrated into practice as collaboration and new ways of working are facilitated. Those new ways of working then need to be captured and the evidence collected in support of a more enlightened commissioning approach that values a wider range of outcomes.


